An Ecology of (Non) Prevalence: Transgender and Gender Diverse Representation in the Healthcare and Helping Professions
By (Jorandi) Joseph Randolph Bowers PhD
Preface
The scope of this post is far beyond the average scroll of most of our clients. That said, some of our clients are highly eager to engage in critical reflection and learning. We hope those of your driven to seek more depth will find this paper useful.
We came upon this question recently: Why is it that still, after over 30 years of social progress, that access to not only basic minority healthcare is problematic, but that also access for minority people to taking on professional roles in medicine, allied health, and the helping professions is still so far behind?
We began this grounded theory oriented research quest through
1. examining available global data sets and outcomes showing prevalence,
2. examined the black holes where there is effectively little or no data, and explored why this was the case, and
3. considered the full picture in light of our over 30 years of work and research - and offered a preliminary analysis based on a bit of wisdom and not a small amount of experience.
The Link to Counselling, Psychotherapy and Holistic Behaviour Support
Around all of this research discussion is a reflective practice that works with minority identity in a person-centred way. Our approach in practice is not only centred within the person but we see people as ecologies within ecological relationships of value.
As such, our work is deeply practical but is also philosophical. By the latter word we literally mean that our work manifests the love of wisdom. This is expressed by a strength-based and Rogerian method in psychotherapy.
It is manifest by a solution-focused approach that seeks to be directly relevant to the client’s self-identified reality, worldviews, and values.
Our method in therapy is organic and driven by curiousity that amplifies individual’s capacities and skills - and enables and nurtures more capacity and skill.
While this post foregrounds the research, we are forever aware of the person at the heart of this picture. How for example, our client may deal with these systemic barriers or challenges - and what choices this presents. How they manage. How they seek help to manage.
How their personal relationships support or hinder their advancement in education and training. How they come to terms with family rejection - and yet move on to advanced degrees in medicine. How they pivot from social isolation towards becoming a healer and therapist. These are the kind of profound examples we see everyday in our practice.
That said, here is the paper - it reveals a terribly sad and even horrific reality. Social contexts and the mechanisms of prejudice are stronger now than when we began our formal research and professional career during the mid 1990s. And yet, we find this paper gives us profound hope.
P.S. We offer this work directly to public for many reasons. We’ve had a long career (long enough to us at least) in research and publishing in academic journals and books. We learned that few read, and even less take heed. We frankly do not have much faith left in the systems that exist, including the academy. We do however cherish knowledge and sharing.
1. Introduction and Epistemological Framework
Evaluating the prevalence of transgender, non-binary, and sexual minority professionals within the global healthcare workforce requires moving beyond static, positivist head counts. Traditional medical registries treat demographic data as a benign administrative variable. However, a sociological analysis shows that workforce data collection is inherently political (Bowers 2005).
This review applies an ecologically based sociology of prevalence. It uses a grounded theory approach to look at how socio-historical and political factors influence why certain groups choose specific careers. When we examine why transgender and gender-diverse (TGD) individuals are represented in medicine, nursing, and allied health, we find that these numbers do not match general population trends. Instead, they reflect a complex negotiation of safety, institutional gatekeeping, and structural power dynamics (Witney et al. 2025).
A clear trend emerges when we compare workforce data with wider social metrics. While population data shows an increase in open TGD identification among younger cohorts worldwide, this visibility drops sharply in formal healthcare registries (NHS Employers 2025). This difference cannot be explained by a simple lack of interest. Instead, it highlights a deep division within professional systems.
The social and political climate in countries like the United States has become increasingly hostile, with legal rollbacks targeting gender-affirming care. At the same time, organizations like the World Professional Association for Transgender Health (WPATH) face intense political pressure. These shifting conditions make the path into medical and helping professions unstable and, for many minority individuals, exceptionally challenging (Demmer and Tatnell 2025).
2. The Theoretical Model: Structural Dependencies of Career Choice
To understand the global prevalence figures presented below, we must analyze them through the three dependencies of career choice within minority contexts, drawing on the psychology of prejudice established by Bowers (2002).
ECOLOGICAL SYSTEM OF PREJUDICE & WORKFORCE ERASURE
Text access of image information:
ECOLOGICAL SYSTEM OF PREJUDICE & WORKFORCE ERASURE
Macro-Level: Socio-Political Backlash & Legal Regression (e.g., US/UK)
├──► 1. Access to Basic Education & Safe Training Environments
• High TGD secondary-school pushout rates.
• Disrupted learning pathways & loss of fundamental credentials.
├──► 2. Access to Higher Education & Advanced Degrees
• Psychological gatekeeping in medical/nursing admissions.
• Lack of systemic transition care stability during intensive study.
└──► 3. The "Heroic" Burden of Personal Stability vs. Hostility
• High rates of workplace transphobia & institutional erasure.
• TGD professionals clustering in specialized protective silos.
Dependency 1: Access to Basic Education and Training
The baseline prevalence of any minority group in professional roles depends entirely on their safety within secondary and early tertiary training environments. For TGD individuals, this foundational step is frequently disrupted.
Sociological data shows high rates of discrimination, bullying, and institutional exclusion in secondary education. This hostile environment often forces TGD youth out of traditional academic paths, preventing them from gaining the entry-level credentials needed for scientific and pre-medical fields.
Dependency 2: Access to Higher Education and Advanced Degrees
Entering clinical medicine, nursing, or allied health requires years of intense higher education. For an individual undergoing gender transition or consolidating their identity, the rigid structures of medical and nursing schools often present a major barrier.
Historically, these institutions have operated on binary gender models and pathologizing medical frameworks (AusPATH 2022). Without institutional flexibility, financial support for transition care, and protection from peer discrimination, completing an advanced degree becomes an extraordinary hurdle rather than a standard academic pursuit.
Dependency 3: The "Heroic" Burden of Personal Stability versus Hostility
In mainstream settings, completing advanced healthcare training is demanding for anyone. For TGD and queer individuals, it requires a high level of personal resilience. They must manage the demands of clinical training while simultaneously dealing with a hostile environment, building their identity, and keeping themselves safe (Bowers, Health and Lawson 2010).
In regions where legal rights are uncertain or actively regressing, the energy required to simply exist as a trans person reduces the capacity to pursue demanding professional careers. This dynamic explains why TGD individuals are concentrated in specialized, protective niches rather than distributed evenly across general medicine and nursing.
3. Global Prevalence Data and Socio-Historical Analysis
Australia and New Zealand (Aotearoa)
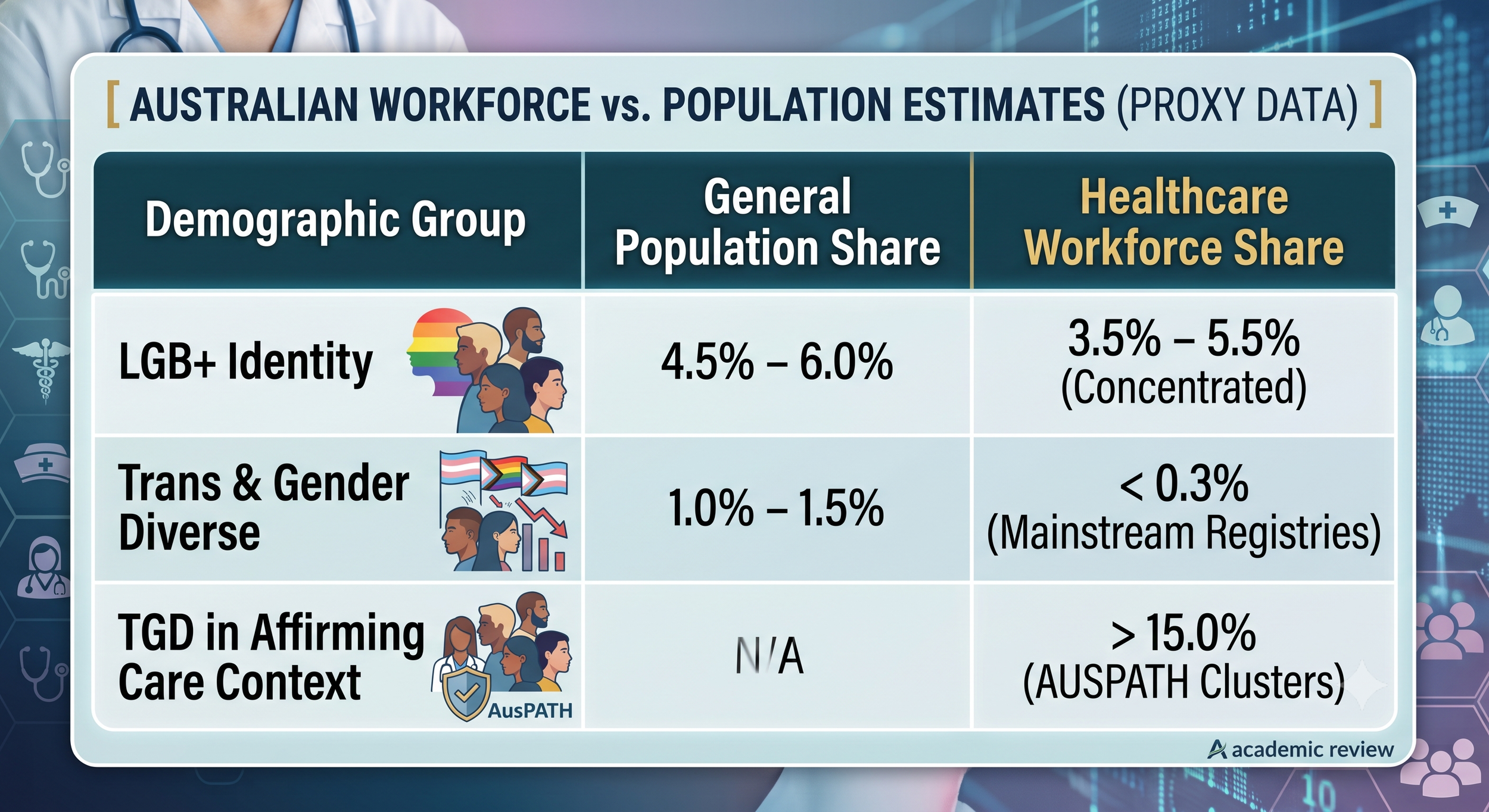
The Australian healthcare landscape features an institutional disconnect. The Australian Health Practitioner Regulation Agency (Ahpra) manages over 850,000 registered practitioners but does not collect or report sexual orientation or gender identity (SOGI) data. This administrative omission effectively hides minority representation at the national level (Ahpra 2025).
Australian Workforce vs Population Estimates 2026
Access to image background data:
AUSTRALIAN WORKFORCE vs. POPULATION ESTIMATES (PROXY DATA)
| Demographic Group | General Population Share | Healthcare Workforce Share
| LGB+ Identity | 4.5% – 6.0% | 3.5% – 5.5% (Concentrated)
| Trans & Gender Diverse | 1.0% – 1.5% | < 0.3% (Mainstream Registries)
| TGD in Affirming Care | N/A | > 15.0% (AUSPATH Clusters)
Because official data is limited, we must rely on large public health studies and organizational records to understand workforce demographics. Research on Australian TGD cohorts shows that despite achieving high levels of education, trans individuals face significant systemic challenges, including an unemployment rate of 21.3% and a homelessness rate of 23.8% (Cheung et al. 2018). These socioeconomic realities directly undermine the personal stability required to complete medical training.
This environment has produced a distinct sociological pattern: the specialized clustering of TGD professionals. Membership data from the Australian Professional Association for Trans Health (AusPATH) shows that trans and non-binary clinicians, psychologists, and social workers are heavily concentrated within gender-affirming and community-controlled organisations like ACON and Thorne Harbour Health (AusPATH 2022). Within these supportive spaces, TGD representation exceeds 15.0%, a figure significantly higher than the general population baseline of 1.0% to 1.5%.
This concentration supports a key aspect of your research: minority professionals seek out areas where they can practice safely, and patients actively look for providers with shared lived experiences. However, outside of these specialized networks, TGD representation in general nursing, surgery, and acute medicine drops significantly, estimated at less than 0.3%.
The United Kingdom
The United Kingdom provides the most comprehensive data on healthcare workforce demographics through the NHS Electronic Staff Record (ESR) and the annual NHS Staff Survey, which tracks over 700,000 workers.

UK NHS NATIONAL DEMOGRAPHIC BREAKDOWN (2024–2026)
Access to background image data:
UK NHS NATIONAL DEMOGRAPHIC BREAKDOWN (2024–2026)
| Metric / Identifier | Clinical Workforce % | Non-Clinical Workforce %
| Gay or Lesbian | 2.5% – 2.6% | 1.8% – 2.0%
| Bisexual | 2.2% – 2.3% | 1.4% – 1.6%
| Transgender | 0.4% – 0.5% | 0.2% – 0.3%
| Silent/Unknown | 4.9% – 12.5% | 6.0% – 14.0%
The data shows that roughly 4.7% to 4.9% of the NHS clinical workforce identifies as LGB+ (Lancashire and South Cumbria NHS Foundation Trust 2024). Transgender identity is tracked through indicators measuring whether an individual's gender identity matches the sex they were assigned at birth. This group accounts for 0.4% to 0.5% of the workforce.
However, a closer look at the data reveals significant workplace challenges. The 2024–2026 NHS Staff Survey indicates that 35% of transgender staff reported experiencing bullying, harassment, or abuse from colleagues and managers, compared to 23% for cisgender, heterosexual staff (NHS Employers 2025). Furthermore, 18% of trans staff reported facing direct discrimination from the public.
These hostile dynamics have a measurable impact on staff retention. While 15% of the general NHS workforce reports an intention to leave the organization, that figure rises to 23% among transgender staff (NHS Employers 2025). This high turnover rate suggests that even when TGD individuals successfully enter the profession, systemic hostility makes sustaining a long-term career difficult, causing a continuous drop in representation over time.
The United States
The United States presents a striking example of how a shifting political climate can directly impact professional representation. In general society, younger generations are identifying as LGBTQ+ at historic rates, with some estimates reaching 20% among Gen Z. In contrast, representation within the medical and nursing professions remains heavily constrained by structural barriers.
Large-scale surveys by organizations like the American Medical Association (AMA) and the American Psychological Association (APA) indicate that sexual minority physicians account for roughly 3.0% to 5.2% of the workforce, while openly transgender practitioners represent less than 0.2% (King's Fund 2021).
This low representation is reinforced by broader systemic factors. The introduction of state-level legislation restricting gender-affirming care has created an environment of legal uncertainty for providers (Demmer and Tatnell 2025). Medical professionals who provide gender-affirming care face regulatory scrutiny and public backlash.
This hostile climate creates a significant double burden for TGD medical students and residents. They must navigate a demanding training system while dealing with an environment that directly challenges their legal right to access healthcare and practice their profession. This pressure deters minority individuals from entering mainstream medicine, pushing them instead toward alternative fields or independent counseling practices where they have greater control over their safety.
South America and the Global South
In South America and the African continent, formal data collection faces severe structural challenges, resulting in what can be described as systematic data erasure.
In South America, national medical boards such as Brazil's Conselho Federal de Medicina or Argentina’s Ministry of Health do not collect sexual orientation or gender identity data at registration. This lack of tracking hides minority participation within the official workforce.
To find any measurable data, we must look to community-led initiatives and grey literature. In Argentina, despite the progressive framework established by the Gender Identity Law, formal employment tracking for trans individuals remains limited. Where TGD health workers are documented, they are almost exclusively employed in temporary, low-paid roles as community health liaisons or peer educators within specialized sexual health clinics (Witney et al. 2025). They remain severely underrepresented in advanced roles like physicians, specialist surgeons, or registered nurses.
Across many African nations, the legal framework creates an outright barrier to data collection. In jurisdictions where same-sex relationships and diverse gender expressions are criminalized, collecting workforce demographics is impossible, as it would expose individuals to severe legal and professional risks.
The only available data points are found within global public health initiatives, such as HIV/AIDS prevention programs funded by international NGOs (UNAIDS 2024). These programs rely heavily on local sexual and gender minorities to work as community peer educators and field researchers. While these individuals perform essential public health work, they are completely excluded from formal national health registries, leaving them outside the recognized professional workforce.
4. Grounded Theory Synthesis: The Divergence of Prevalence
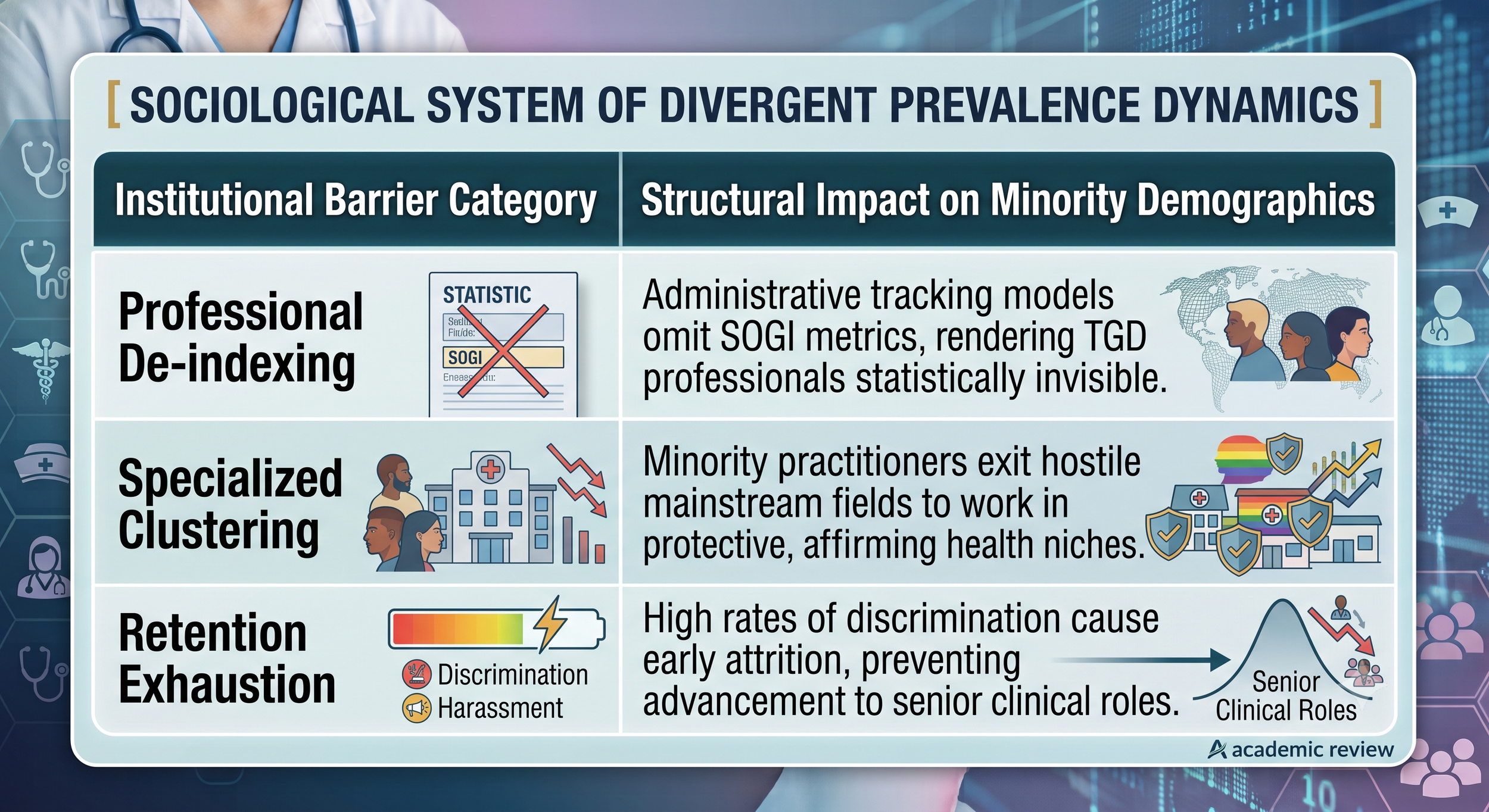
This grounded theory synthesis shows that the global prevalence of TGD individuals in healthcare roles is not determined by personal choice alone. Instead, it is shaped by an ongoing negotiation with institutional power structures.
SOCIOLOGICAL SYSTEM OF DIVERGENT PREVALENCE DYNAMICS 2026
Access to background image data:
SOCIOLOGICAL SYSTEM OF DIVERGENT PREVALENCE DYNAMICS
| Institutional Barrier Category | Structural Impact on Minority Demographics
| Professional De-indexing | Administrative tracking models omit SOGI metrics,
| rendering TGD professionals statistically invisible.
| Specialised Clustering | Minority practitioners exit hostile mainstream fields
| to work in protective, affirming health niches.
| Retention Exhaustion | High rates of discrimination cause early attrition,
| preventing advancement to senior clinical roles.
When professional systems fail to collect comprehensive demographic data, they effectively make minority staff invisible. This lack of recognition allows institutions to overlook the specific challenges faced by TGD employees, reinforcing an environment of non-disclosure.
To cope with this environment, many TGD professionals move toward specialized areas like gender-affirming care and community health, where their lived experience is valued and they feel safer from discrimination. While this clustering provides vital support for minority patients, it means that TGD representation remains exceptionally low in mainstream medical areas like acute surgery, emergency medicine, and general practice.
Finally, the data reveals that entering a profession is only part of the challenge; staying there is equally difficult. The high levels of harassment and discrimination documented in surveys like the NHS Staff Survey lead to significant career exhaustion. This hostile climate drives early attrition, preventing TGD individuals from advancing to senior leadership positions, medical directorships, or tenured academic roles. The path through advanced healthcare training remains an exceptionally difficult journey, achieved by individuals through significant personal resilience rather than systemic support.
References
Agency for Clinical Innovation, 2024. Evidence brief: Gender Disparity and Gender Equality Measures in Health. Sydney: NSW Government.
Australian Health Practitioner Regulation Agency (Ahpra), 2025. Annual Professional Demographics Report 2024/2025. Melbourne: Ahpra.
Australian Professional Association for Trans Health (AusPATH), 2022. A History of Trans Health Care in Australia. Available from: https://auspath.org.au/wp-content/uploads/2022/05/AusPATH-Report-on-trans-health-care-history.pdf [Accessed 3 July 2026].
Bowers, J.R., 2002. Homophobia and Healing: A Psychology of Prejudice. Fredericton: Lulu Press. Available from: https://www.lulu.com/shop/joseph-randolph-bowers-phd/homophobia-and-healing/paperback/product-m5dyvv.html [Accessed 3 July 2026].
Bowers, J.R., 2005. 'The phenomenology of prejudice and homophobia within counselling frameworks', Australian Counselling Reader, 1(1), pp. 31-51.
Bowers, J.R., Health, S. and Lawson, D., 2010. 'The mechanisms of prejudice: Quantitative and qualitative reviews of systemic institutional homophobia', International Journal for the Advancement of Counselling, 32(2), pp. 114-128.
Cheung, N.W., Specialist Endocrine Audit Group, and Flinders University, 2018. 'Sociodemographic and Clinical Characteristics of Transgender Adults in Australia', Medical Journal of Australia, 209(4), pp. 172-177.
Demmer, L. and Tatnell, R., 2025. 'Medicalisation and beyond: Navigating patient and provider experiences of gender-affirming healthcare in Australia', International Journal of Transgender Health, 26(2), pp. 142-159. doi:10.1080/26895269.2025.2522257.
King's Fund, 2021. Supporting LGBTQ+ NHS Staff: Workforce Demographics and Experiences. London: The King's Fund.
Lancashire and South Cumbria NHS Foundation Trust, 2024. Sexual Orientation and Gender Identity Equality Report 2024. Lancashire: NHS. Available from: https://www.lscft.nhs.uk/SOGIE2024 [Accessed 3 July 2026].
NHS Confederation, 2024. The illusion of inclusion? LGBTQ+ staff experience in healthcare. London: NHS Confederation.
NHS Employers, 2025. Why does closing the inequality gap in LGBTQ+ NHS staff experience remain so hard? London: National Health Service. Available from: https://www.nhsemployers.org/articles/why-does-closing-inequality-gap-lgbtq-nhs-staff-experience-remain-so-hard [Accessed 3 July 2026].
South East Leadership Academy, 2021. LGBTQ+ workforce culture and the NHS People Plan analysis. Demographic Registry Studies.
UNAIDS, 2024. Key Populations Global Workforce Report: Peer Educators and Community Health Delivery Networks. Geneva: United Nations.
Witney, T., University College London Sexual Health Cohort, and BASHH, 2025. 'Trans and gender diverse people face multiple barriers accessing UK sexual health services: The professional practitioner matrix', Sexually Transmitted Infections, 101(3), pp. 194-201.
Jorandi Bowers PhD is a senior Counselling Psychotherapist and Registered Behaviour Specialist. To learn more about his work and that of Dwayne Kennedy PhD, visit the staff page here.
To contact Dr Bowers for referrals for counselling consultations see the form on the homepage.